Bruce P. Robinson, MD

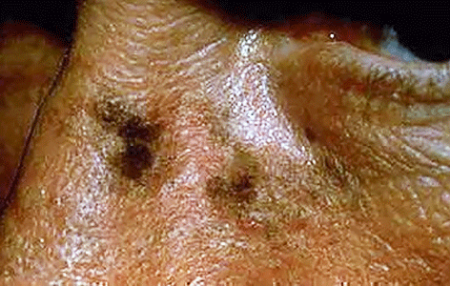
Age spots are small, flat dark areas on the skin. They vary in size and usually appear on areas exposed to the sun, such as the face, hands, shoulders and arms. Age spots are also called sunspots, liver spots and solar lentigines.
Age spots can look like cancerous growths. True age spots don't need treatment, but they are a sign the skin has received a lot of sun exposure and are an attempt by your skin to protect itself from more sun damage. You can help prevent age spots by regularly using sunscreen and avoiding the sun.
Age spots may affect people of all skin types, but they're more common in adults with light skin. Unlike freckles, which are common in children and fade with no sun exposure, age spots don't fade.
Age spots don't require medical care. Have your doctor look at spots that are black or have changed in appearance. These changes can be signs of melanoma, a serious form of skin cancer.
It's best to have any new skin changes evaluated by a doctor, especially if a spot:
Age spots are caused by overactive pigment cells. Ultraviolet (UV) light speeds up the production of melanin, a natural pigment that gives skin its color. On skin that has had years of sun exposure, age spots appear when melanin becomes clumped or is produced in high concentrations. Also, the use of commercial tanning lamps and beds can cause age spots.
We offer a range of advanced laser therapies tailored to the type and depth of discoloration, whether you’re dealing with brown spots, melasma, sun damage, or red marks from acne or rosacea. Each treatment is selected based on your unique skin tone, condition, and goals.
Lasers for Brown Spots, Melasma & Sun Damage:
These lasers use ultra-short pulses to break up unwanted pigment while minimizing damage to surrounding skin, ideal for darker skin tones.
Q-switched Nd:YAG Laser: Targets deep pigmentation, including melasma and post-inflammatory hyperpigmentation (PIH), with precision and safety for all skin tones.
Fractional Lasers: These versatile lasers treat pigmentation and improve overall skin quality by stimulating collagen production and resurfacing the skin. Great for: PIH (post inflammatory hyperpigmentation), sun damage, acne scarring, uneven tone, and texture.
Vascular Lasers:
Specialized for redness and pink-toned PIH (post inflammatory hyperpigmentation), especially from acne or rosacea.
Vbeam (Pulsed Dye Laser):
Targets blood vessels to reduce red marks, flushing, and inflammation. A gentle, effective option for sensitive or reactive skin types.
Each laser treatment is customized to your skin’s needs to ensure safe, effective results. During your consultation, we’ll determine the best approach—often combining laser therapy with topical treatments to maximize improvement and minimize recurrence.
For brown marks on deeper skin tones, we use a combination of hydroquinone, kojic acid, Vitamin C, and AHAs to gently and effectively lighten dark spots while brightening and smoothing the skin.
These clinically proven ingredients work synergistically to visibly brighten, lighten, and tighten the skin, revealing a more even, radiant complexion.
JAS Anti - Aging TRIO, expertly formulated to replenish, exfoliate, and restore your skin’s natural glow.
To help avoid age spots and new spots after treatment, follow these tips for limiting your sun exposure:
⚠️ Important
Always see a board-certified dermatologist or laser specialist, especially if you have darker skin.
Sun protection is non-negotiable—exposure after treatment can trigger new pigment.
If you are tired of looking older or want the spots removed, schedule a laser consultation and restore your skin to its natural beauty. Our Cosmetic Consultation Reimbursement policy is offered to all patients. Schedule an office visit to discuss your concerns and skincare goals with Dr. Robinson and the office visit cost will be applied to the future cost for the "consulted procedure". The "consulted procedure" must be completed within 30 days of your consult visit.
Birthmarks are abnormalities of the skin that are present when a baby is born.
A birthmark can be red or brown.
A red or vascular birthmark is made up of dilated blood vessels. Two types are hemangiomas and port-wine stains. Although they can resolve spontaneously on their own, some can cause deformities and become more purple in color. With the advent of laser treatment, the Nevus Flameus can be cleared and subsequent deformities prevented.
A Nevus of Ota, Nevus of Ito and Mongolian spot are brown to bluish birthmarks that usually occur around the eye, shoulder and trunk respectively. Given their size and location patients often consider them cosmetically unacceptable, using the Medlite Nd:Yag laser these birthmarks can be treated effectively with excellent results.
An atypical nevus or dysplastic nevus (mole) is a benign growth that may share some of the features of a melanoma, but is NOT a melanoma or any other form of cancer. The presence of an atypical nevus, however, may increase the risk of developing a melanoma, or be a marker for it. A single atypical nevus may indicate a small risk; this risk increases with the number of atypical nevi present.
An atypical nevus can vary in appearance. Since it has the ABCDE features of a melanoma, it is important ot have a dermatologist examine all moles.
Asymmetry - One half does not match the other half in size, shape, color, or thickness.
Border irregularity - The edges are ragged, scalloped, or poorly defined.
Color - The pigmentation is not uniform. Shades of tan, brown, and black are present. Dashes of red, white, and blue add to the mottled appearance.
Diameter - While melanomas are usually greater than 6mm in diameter (the size of a pencil eraser) when diagnosed, they can be smaller. If you notice a mole different from others, or one which changes, itches, or bleeds (even if it is small), you sould see a dermatologist.
The lifetime risk of a person in the United States developing melanoma is 1 in 75. A patient with one to four atypical nevi without a personal or family history of melanoma is at a slightly higher risk than the general population. The risk of developing melanoma is higher if a patient with atypical nevi has a personal or family history of melanoma. A patient who has multiple atypical and normal nevi (moles) may have Familial Atypical Nevus Syndrome, and is at an increased risk for developing a melanoma, especially if a relative had melanoma.
Where and when do atypical nevi occur?
Atypical nevi begin to appear at puberty and can occur anywhere on the body, but are more common in sun-exposed areas, the back, and the legs.
Since an atypical nevus is not the same as a melanoma, it does not need to be treated aggressively but should be observed for changes, biopsied, or conservatively excised.
Familial Atypical Nevus Syndrome
The National Institute of Health Consensus Conference defines the Familial Atypical Nevus Syndrome as those persons meeting the following criteria:
It is important for people with Familial Atypical Nevus Syndrome to have a full body screening from a dermatologist every three to twelve months beginning with the onset of puberty. The dermatologist might also recommend regular ophthalmologic examinations, baseline skin photography, or regular screenings of relatives to permit early detection and treatment of melanoma since detection in the early stages has a much higher cure rate.
People with Familial Atypical Nevus Syndrome should also examine their own skin every month. When performing self-examinations, be aware of any lesions that appear to change in size, color, and/or shape. If a change has occurred, bring this to the attention of a dermatologist immediately. Information on the early signs of melanoma is available from the dermatologist or the American Academy of Dermatology.
Prevention of Melanoma
Alopecia areata (AA) causes hair loss in small, round patches that may go away on their own, or may last for many years. Nearly 2% of the U.S. population (about four million people) will develop AA in their lifetime. Some people with AA (about 5%) may lose all scalp hair (alopecia totalis) or all scalp and body hair (alopecia universalis). It is an autoimmune disease, in which for unknown reasons your immune system attacks your own hair follicles, (where the hair grows from), resulting in damage that leads to hair loss anywhere on the body. Typically, it affects small patches of hair so, it may go completely unnoticed. However, more patches of hair loss could develop close together, making it more noticeable.
AA occurs world-wide in both genders and in every ethnic group. Children and young adults are most frequently affected, but persons of all ages are susceptible. One in five persons with AA has a family member who also has the disease.
AA usually begins with one or more small, round, coin-size, bare patches. It is most common on the scalp, but can involve any hair-bearing site on the body including eyebrows, eyelashes, and beards. Hair may fall out and regrow with the possibility of full hair regrowth always present. AA usually has no associated symptoms, but there may be minor discomfort or itching prior to developing a new patch. Nails may have tiny pinpoint dents, ridges, become brittle and may, in rare instances, become distorted.

AA is not contagious. It is an autoimmune disease in which the body's immune system attacks itself, in this case, the hair follicles. The cause is not known. A person's particular genetic makeup combined with other factors triggers AA.
The main types are:
Alopecia areata: Alopecia is the medical term for bald. Areata means patchy. This patchy baldness can develop anywhere on the body, including the scalp, beard area, eyebrows, eyelashes, armpits, inside your nose, or ears.
Alopecia totalis: The person loses all hair on the scalp, so the scalp is completely bald.
Alopecia universalis: The person loses all hair, leaving the entire body hairless. This is rare.
Although your dermatologist may know by examining your scalp that you have AA, occasionally, a scalp biopsy is helpful in confirming the diagnosis.
Because there are so many reasons for hair loss, testing is sometimes necessary to make sure alopecia areata is the cause of your hair loss.
A blood test can look for other diseases caused by the immune system. Sometimes, other tests are necessary.
AA is not a symptom of a serious disease and usually occurs in otherwise healthy individuals. Persons with AA may have a higher risk of atopic eczema, asthma, and nasal allergies, as well as other autoimmune diseases such as thyroid disease (Hashimoto's thyroiditis), and vitiligo. Family members may also have atopic eczema, asthma, nasal allergies, or autoimmune diseases (i.e. insulin-dependent diabetes, rheumatoid arthritis, thyroid disease, or systemic lupus erythematosus).

Yes, it is likely that the hair may regrow, but it may fall out again. The course of the disease varies from person to person, and no one can predict when the hair might regrow or fall out again. This unpredictability of AA, and the lack of control over it, makes this condition frustrating. Some people lose a few patches of hair, the hair regrows, and the condition never returns. Other people continue to lose and regrow hair for many years. The potential for full regrowth is always there, even in people who lose all the hair on their scalp and body (alopecia totalis/universalis). Hair could regrow white or fine, but the original hair color and texture may return later.
The good news is that many causes of hair loss can be managed when caught early and further loss can usually be slowed or prevented.
Corticosteroids are anti-inflammatory drugs that suppress the immune system. They can be given as injections into the areas of hair loss, rubbed topically into affected areas or taken orally as pills.
Oral Minoxidil is by prescription only. Dermatologists began using low-dose oral minoxidil for hair loss after noticing the side effects of the high-dose version of the drug used to treat high blood pressure increased hair growth. The efficacy of 5mg oral minoxidil for men with androgenetic alopecia was tested. Researchers concluded that 43% of the patients had excellent results in hair growth. Typically, people prefer oral to topical. They find it easier and more convenient to take the medication orally, may be able to save money with an oral minoxidil prescription and prefer not to have residue on their hair.
Topical Minoxidil 5% Solution aka Rogaine solution or foam is available over the counter. Effectiveness of topical Minoxidil works for about 2 out of 3 men. It's most effective if you're under age 40 and have only recently started to lose your hair. How to use it: Twice a day, when your hair is dry, apply minoxidil on your scalp where the hair has started to thin. Minoxidil can help maintain the regrowth after you stop applying the corticosteroid. It has few side effects, so it’s considered a good option for children. New hair growth may appear in about 12 weeks.
PRP (platelet-rich plasma) therapy for hair loss is a three-step medical treatment in which a person’s blood is drawn, processed, and then injected into the scalp.
PRP injections trigger natural hair growth and maintain it by increasing blood supply to the hair follicle and increasing the thickness of the hair shaft. Sometimes this approach is combined with other hair loss procedures or medications.
PRP therapy is a three-step process. Most PRP therapy requires three treatments 4–6 weeks apart.
Maintenance treatments are required every 4–6 months.
Your blood is drawn — typically from your arm — and put into a centrifuge (a machine that spins rapidly to separate fluids of different densities).
After about 10 minutes in the centrifuge, your blood will have separated into in three layers:
The platelet-rich plasma is drawn up into a syringe and then injected into areas of the scalp that need increased hair growth.
There hasn’t been enough research to prove whether PRP is effective. It’s also unclear for whom — and under what circumstances — it’s most effective.
Wigs, caps, hats, or scarves are important options. Wearing a head covering does not interfere with hair regrowth. This may be a good choice for people with extensive scalp hair loss who do not have enough hair to cover it.
The emotional aspects of living with hair loss can be challenging, especially in a society that regards hair as a sign of youth and good health. It is reassuring that alopecia areata does not affect general health, and should not interfere with your ability to achieve all of your life goals at school, in sports, in your career, and in raising a family.
The National Alopecia Areata Foundation, the NAAF, is a great resource for support, treatment & education.
Schedule an appointment to see which treatment or combination of treatments is the best choice for you.
An actinic keratosis, is a rough, scaly patch on the skin that develops from years of sun exposure. It's often found on the face, lips, ears, forearms, scalp, neck or back of the hands. These represent pre-cancerous growths that can become skin cancer if left untreated.
If you find a spot or growth on your skin that you think could be an actinic keratosis (AK), it’s time for a thorough skin exam. Should you have an AK, an accurate diagnosis and treatment can:
Most people who have AKs (or think they may have an AK) see a dermatologist. This is actually one of the most common conditions that dermatologists diagnose and treat.
When you see a board-certified dermatologist about AKs, your dermatologist will:
If you have one or more AKs on your skin, a board-certified dermatologist can often diagnose you by looking carefully at your skin. While examining your skin, your dermatologist will also look for signs of skin cancer. People who have skin that’s been badly damaged by ultraviolet (UV) light develop AKs and have a higher risk of getting skin cancer.
If you have one or more AKs, your dermatologist will talk with you about whether to treat these precancerous skin growths. Usually, treatment is recommended.
For a few people, a dermatologist may recommend frequent skin exams rather than treatment. Skin exams are recommended for patients who are frail and may find it hard to tolerate treatment. To be effective, treatment must destroy the AKs. When this happens, your skin will feel raw. It may be red and swollen for a brief time.
The treatment that is right for you depends on several considerations, including:
If you have one or a few AKs, a procedure that your dermatologist can perform during an appointment may be the preferred treatment.
You can often complete treatment in 1 or 2 office visits. The procedures that dermatologists use to treat AKs include:
Some people develop a few AKs, which can often be cleared with treatment.
If you have many AKs, it’s a good idea to be under a dermatologist’s care. Your skin has been severely damaged by UV light, so it’s likely you’ll continue get new AKs. You may also develop skin cancer. Your dermatologist can watch for signs of new AKs and skin cancer. When found early and treated, skin cancer is highly treatable.
Your dermatologist will tell you how often to return for check-ups. Some people need a check-up once or twice a year. If you have a weakened immune system or a rare condition that greatly increases your risk of developing AKs and skin cancer, you may need to see your dermatologist every 8 to 12 weeks.
Keep every appointment. If skin cancer develops, the sooner it is found and treated, the better your outcome.
Self-care also plays a key role in your outcome. The right self-care can help to prevent new AKs and skin cancer.


Acne is a skin condition which has plugged pores (blackheads and whiteheads), inflamed pimples (pustules), and deeper lumps (nodules). Acne occurs on the face, as well as the neck, chest, back, shoulders, and upper arms. Although most teenagers get some form of acne, adults in their 20's, 30's, 40's, or even older, can develop acne. Often, acne clears up after several years, even without treatment. Acne can be disfiguring and upsetting to the patient. Untreated acne can leave permanent scars; these may be treated by your dermatologist in the future. To avoid acne scarring, treating acne is important.
Acne is not caused by dirt. Testosterone, a hormone which is present in both males and females, increases during adolescence (puberty). It stimulates the sebaceous glands of the skin to enlarge, produce oil, and plug the pores. Whiteheads (closed comedones), blackheads (open comedones), and pimples (pustules) are present in teenage acne.
Early acne occurs before the first period and is called prepubertal acne. When acne is severe and forms deep "pus-filled" lumps, it is called cystic acne. This may be more common in males. Adult acne develops later in life and may be related to hormones, childbirth, menopause, or stopping the pill. Adult women may be treated at the period and at ovulation when acne is especially severe, or throughout the entire cycle. Adult acne is not rosacea, a disease in which blackheads and whiteheads do not occur.
Acne has nothing to do with not washing your face. However, it is best to wash your face with a mild cleanser and warm water daily. Washing too often or too vigorously may actually make your acne worse.
Acne is not caused by foods. However, if certain foods seem to make your acne worse, try to avoid them.
Wear as little cosmetics as possible. Oil-free, water-based moisturizers and make-up should be used. Choose products that are "non-comedogenic" (should not cause whiteheads or blackheads) or "non-acnegenic" (should not cause acne). Remove your cosmetics every night with mild soap or gentle cleanser and water.
A flesh-tinted acne lotion containing acne medications can safely hide blemishes. Loose powder in combination with an oil-free foundation is also good for cover-up.
Shield your face when applying sprays and gels on your hair.
Control of acne is an ongoing process. All acne treatments work by preventing new acne breakouts. Existing blemishes must heal on their own, and therefore, improvement takes time. If your acne has not improved within two to three months, your treatment may need to be changed. The treatment your dermatologist recommends will vary according to the type of acne.
Occasionally, an acne-like rash can be due to another cause such as make-up or lotions, or from oral medication. It is important to help your dermatologist by providing an updated history of what you are using on your skin or taking internally.
Many non-prescription acne lotions and creams help mild cases of acne. However, many will also make your skin dry. Follow instructions carefully.
Re-think your skin health. Hydrafacial MD, - * Acne Facial, is highly effective for anyone suffering from oily and/or acne-prone skin. It visibly reduces redness, enlarged pores, hyperpigmentation, utilizing LED blue light killing acne causing bacteria. HydraFacial MD - Hydradermabrasion is the latest, non-invasive, "gentle" skin resurfacing and complexion treatment. The immediate, noticeable, long lasting results are achieved with zero downtime and without any discomfort. You can return to school, work, social life, or exercise right after your procedure. HydraFacial MD uses a uniquely shaped spiral tip and patented vortex fusing technology to gently cleanse, exfoliate, and extract, removing impurities and dead skin cells while hydrating the skin and adding antioxidant protection simultaneously.
Acne scars no longer have to be lived with forever. Often occurring on the face, back and chest these scars can now be treated with a variety of lasers (Fraxel®, V-Beam), subcission or chemical peels. These treatments require no social downtime and can be performed on all skin colors.
You're more likely to get Lyme disease if you live or spend time in grassy and heavily wooded areas where ticks carrying Lyme disease thrive. It's important to take common-sense precautions in tick-infested areas.
Where you live or vacation can affect your chances of getting Lyme disease. So can your profession and the outdoor activities you enjoy. The most common risk factors for Lyme disease include:


A small, red bump, similar to the bump of a mosquito bite, often appears at the site of a tick bite or tick removal and resolves over a few days. This normal occurrence doesn't indicate Lyme disease.
However, these signs and symptoms can occur within a month after you've been infected:

If untreated, new signs and symptoms of Lyme infection might appear in the following weeks to months. These include:
Several weeks after infection, some people develop:
If you've been bitten by a tick and have symptoms, only a minority of tick bites lead to Lyme disease. The longer the tick remains attached to your skin, the greater your risk of getting the disease. Lyme infection is unlikely if the tick is attached for less than 36 to 48 hours.
If you think you've been bitten and have signs and symptoms of Lyme disease — particularly if you live in an area where Lyme disease is common — contact your doctor. Treatment for Lyme disease is more effective if begun early.
Visit your doctor even if signs and symptoms disappear — the absence of symptoms doesn't mean the disease is gone. Untreated, Lyme disease can spread to other parts of your body for several months to years after infection, causing arthritis and nervous system problems. Ticks can also transmit other illnesses, such as babesiosis and Colorado tick fever.
The best way to prevent Lyme disease is to avoid areas where deer ticks live, especially wooded, bushy areas with long grass. You can decrease your risk of getting Lyme disease with some simple precautions:
Psoriasis is a common, chronic, long term, relapsing skin condition where the skin cells are made to quickly often resulting in itchy silvery scaling patches that causes a rash, most commonly on the knees, elbows, trunk and scalp. It can be painful, interfere with sleep and make it hard to concentrate. The condition tends to go through cycles, flaring for a few weeks or months, then subsiding for a while.
Common signs and symptoms of psoriasis include:
There are several types of psoriasis, each of which varies in its signs and symptoms:
Many people who are predisposed to psoriasis may be free of symptoms for years until the disease is triggered by some environmental factor. Common psoriasis triggers include:
Anyone can develop psoriasis. About a third of instances begin in childhood. These factors can increase the risk of developing the disease:
If you have psoriasis, you're at greater risk of developing other conditions, including:
If you suspect that you may have psoriasis, see your health care provider. Also seek medical care if your condition:





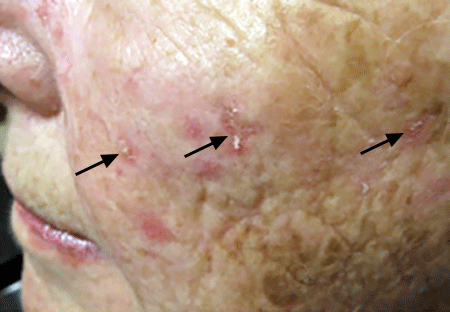
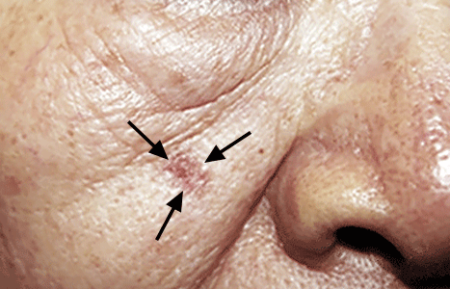
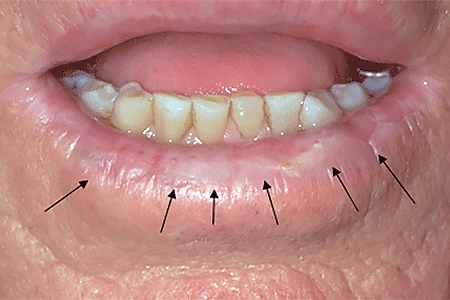
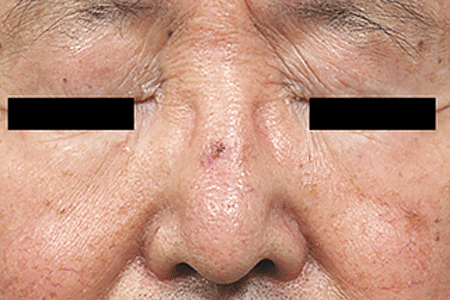
Basal cell carcinoma is the most common form of cancer worldwide. In the vast majority of cases, it is thought to be caused by exposure to the harmful ultraviolet rays of the sun. It is becoming more common, perhaps because people may be spending more time outdoors. Some believe that the decrease in the ozone layer is allowing more ultraviolet radiation from the sun to reach the earth's surface. Basal cell cancer does not usually metastasize or travel in the bloodstream; rather it infiltrates the surrounding area destroying tissue. For this reason, basal cell cancer should be treated promptly by your dermatologist with dermatologic surgical techniques.

Basal cell cancer most often appears on sun-exposed areas such as the face, scalp, ears, chest, back, and legs. These tumors can have several different forms. The most common appearance of basal cell cancer is that of a small dome-shaped bump that has a pearly white color. Blood vessels may be seen on the surface. Basal cell cancer can also appear as a pimple-like growth that heals, only to come back again and again. A less common form called morpheaform, looks like a smooth white or yellowish waxy scar. A very common sign of basal cell cancer is a sore that bleeds, heals up, only to recur again.
If you have a sore that doesn't heal, or that looks like any of the growths pictured here, you should make an appointment with your dermatologist for evaluation. After the dermatologist examines the growth, he or she will decide whether or not to perform a biopsy. A biopsy is a simple procedure done in the office under local anesthesia. The dermatologist will first inject a small amount of anesthesia similar to the type used by your dentist. After the area is numb, the dermatologist will remove a small sample of the growth or use a small cookie-cutter device to do a "punch" biopsy. A bandage will then be placed on the wound and you will receive instructions on how to care for the wound. The area will heal over five to seven days. There are several different kinds of basal cell cancer. The biopsy results will indicate whether or not you have a basal cell cancer and what kind of basal cell cancer it is. In some cases, if the basal cell cancer is very thin and present only on the surface of the skin, your dermatologist may choose to perform the biopsy and treat the skin cancer at the same time.

Your dermatologist will discuss with you the various dermatologic surgical options should your growth prove to be a basal cell cancer. Your dermatologist may use a method called electrodesiccation and curettage. In this procedure the surface of the skin cancer is removed and the base of the skin cancer is gently burned or "cauterized" with an electric needle. When this is done there is often no need for further treatment. Simple surgical excision, in which the skin cancer is cut out and the skin sewn together using dermatologic cosmetic surgical techniques will often be recommended. In this case, the specimen is examined under a microscope after the procedure to determine that all the skin cancer has been removed. Other treatment methods, such as cryosurgery, radiation therapy, and laser surgery may be used in specific circumstances. In certain situations, your dermatologist may refer you for a specialized technique called Mohs micrographically controlled surgery. In this method, performed by specially trained dermatologic surgeons, the skin cancer is removed under local anesthesia in an office setting and microscopic sections are prepared on slides while you wait. Your Mohs surgeon examines the slides to determine if most of the cancer cells have been removed. If not additional layers are taken until the cancer is completely excised. The advantage of this technique is that a minimum amount of tissue is removed and all the edges of the specimen are carefully studied. This method has a high cure rate, but is not required for all skin cancers. In general, most dermatologists agree that recurrent skin cancers, that is skin cancers that were previously treated and have come back, incompletely removed skin cancers, large skin cancers, and skin cancers in cosmetically important areas, may benefit from the Mohs technique. After the skin cancer has been removed using this method, it maybe allowed to heal naturally or reconstructive surgery using a skin flap or skin graft maybe performed.

Because the vast majority of skin cancers occur on the face, many patients are understandably concerned about the cosmetic outcome. If the skin cancer is small, conservative methods usually produce an excellent cosmetic result. If the skin cancer requires more specialized treatment such as Mohs surgery, reconstructive options are available that, in most cases, result in an excellent cosmetic outcome.

Some people wonder whether it is worth treating basal cell cancer at all since it doesn't metastasize or travel in the bloodstream to other organs. It is important to remember that basal cell cancer is in fact a cancer, and will continue to grow locally unless treated. Basal cell cancer does not spontaneously go away on its own. In addition, if the skin cancer is located near important organs such as the eyes, ears, and nose, or is growing near a nerve, serious problems can arise if the skin cancer is neglected.
If you have already had one basal cell cancer studies have shown that you are at a 40% risk of getting a second basal cell cancer within five years. It is important to follow closely with your dermatologist and be alert to any non-healing sores that develop on your skin.
Individuals who have had multiple basal cell cancers or other skin cancers, such as squamous cell, are at an increased risk for melanoma. It is important to have a full body skin examination at least once a year to check for abnormal moles which could be precursors to melanoma or melanoma itself. It is also important to know that basal cell cancer does not turn into melanoma.
Because basal cell cancer is caused by ultraviolet radiation from the sun in the vast majority of cases, proper sun protection may help to prevent the development of further basal cell cancers. Because 85% of lifetime sun exposure is acquired in childhood by age 18, careful sun protection in children may effectively prevent basal cell cancer later in life. Follow these simple steps from your dermatologist and dermatologic surgeon: 1. Apply sunscreen with a sun protection factor of 15 or greater while outdoors 2. Wear a broad-brimmed hat and sun protective clothing 3. Avoid the sun between 10:00 a.m. and 4:00 p.m.
Many people wonder how often they have to reapply sunscreen. In general, if you are active outdoors, it is quite reasonable to apply sunscreen every 1 1/2 hours. As long as you practice good sun protection habits and enjoy the sun in moderate amounts you should be able to minimize the chances of developing basal cell cancer.

