Bruce P. Robinson, MD

Dry skin (eczema) and Keratosis Pilaris, are common disorders of the skin. Keratosis Pilaris (KP) is characterized by rough epidermal regions and patches of small acne-like bumps that typically appear on the upper arms, thighs, buttocks, and cheeks. Doctors typically identify KP in patients who complain of the appearance of “gooseflesh,” “goose bumps,” or “chicken skin” on various body parts. These bumps can be white, tan, or red in color. The condition is caused by the keratinization (or cellular “hardening”) of the skin’s hair follicles.Keratosis Pilaris often runs in families. Although its poses no serious medical threat, KP is often considered cosmetically displeasing. During particularly violent outbreaks, many KP sufferers report persistent itching in the affected area. The disorder can affect people of all ages, but most patients find that the major symptoms of KP disappear completely by age 30.
Because the general public is unaware of KP as a medical condition, many individuals are diagnosed with the condition when visiting dermatologists and other medical professionals for unrelated skin conditions. KP is often seen in patients with other epidermal disorders such as dry skin and eczema. If moisturizing doesn't help make an appointment as prescription strength treatment may be needed.
A cyst is a closed sac with a defined membrane and division on the nearby tissue.
Cysts may contain fluid, air or semisolid material. Parasites — such as trichinosis, dog tapeworm and echinococcus. Cysts are typically benign growths that consist of a wall that makes the contents. Often these bumps are cosmetically unacceptable or patients desire removal in the event they may rupture. Although cysts can remain intact for a lifetime, may go away on their own.There is also the risk of rupturing, which can lead to a great deal of inflammation, pain and infection. This necessitates surgical excision.
Sebaceous / Epidermoid Cysts are typically a common, noncancerous type of cyst. Sebaceous cysts arise from sebaceous glands that secrete oily matter that lubricates the hair and skin. These cysts, which may be hereditary, are caused when glands or hair follicles become blocked. Trauma to the skin is another likely cause of a cyst. These cysts appear as small bumps beneath the skin. Although they can occur almost anywhere on the body, they typically appear on the face, neck and trunk. A foul odor may be secreted from the outside skin of the cyst. Sebaceous cysts grow slowly and usually are not painful; thus, treatment is rarely needed. However, options are available if these cysts become painful or have an unacceptable appearance.
There are three common cyst removal techniques specifically for sebaceous cysts — conventional wide excision, minimal excision and punch biopsy excision.
Lastly, these cysts typically appear on the scalp which originate in the skin and hair follicles, may cause lumps under the skin, but often do not require surgical removal.
"OUCH! What Bit Me?"
Sometimes it’s easy to tell what bit you: maybe you reach down to swat at the bug and catch a glimpse of it. Sometimes though, it’s harder to tell. You might not notice the bite as it’s happening. Instead you don’t even realize you’ve been bitten until the spot starts to itch.
Although most bug bites and stings are harmless, some can be dangerous. This is especially true if you are allergic to the bug’s venom, or if the bug is carrying a disease. Most bug bites and stings can be safely treated at home with topical medication. However, sometimes a bug bite or sting could turn into something serious – particularly if you have been bitten or stung by many insects at the same time.
In the United States, it’s common to experience a bite or sting from the following types of bugs:
When weather permits, wear long sleeves and pants. They can add an extra layer of protection between you and your exposed skin. Light-colored clothing makes ticks easier to spot. Do a quick clothing and body check for ticks once you get inside.
Remember, insect repellants are your friend. The best ones contain DEET, like DEEP Woods OFF or ones that contain picaridin. Be sure to use any insect repellants according to the directions on the label.
For insect bites and stings that itch, you can put an ice pack on the spot and/or use an over-the-counter itch cream; for example, hydrocortisone. You may choose to instead take an oral antihistamine. Ice packs can also reduce swelling.
It’s important to pay attention to your symptoms. If you feel tired all the time, you have a headache, fever or body aches, or you develop a rash after a bug bite, see a board-certified dermatologist immediately.
Go to the emergency room immediately if you experience any of the following symptoms after a bug bite or sting:
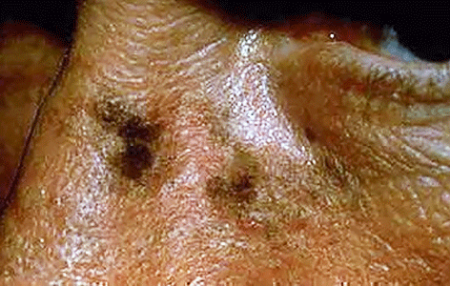
Age spots are small, flat dark areas on the skin. They vary in size and usually appear on areas exposed to the sun, such as the face, hands, shoulders and arms. Age spots are also called sunspots, liver spots and solar lentigines.
Age spots can look like cancerous growths. True age spots don't need treatment, but they are a sign the skin has received a lot of sun exposure and are an attempt by your skin to protect itself from more sun damage. You can help prevent age spots by regularly using sunscreen and avoiding the sun.
Age spots may affect people of all skin types, but they're more common in adults with light skin. Unlike freckles, which are common in children and fade with no sun exposure, age spots don't fade.
Age spots don't require medical care. Have your doctor look at spots that are black or have changed in appearance. These changes can be signs of melanoma, a serious form of skin cancer.
It's best to have any new skin changes evaluated by a doctor, especially if a spot:
Age spots are caused by overactive pigment cells. Ultraviolet (UV) light speeds up the production of melanin, a natural pigment that gives skin its color. On skin that has had years of sun exposure, age spots appear when melanin becomes clumped or is produced in high concentrations. Also, the use of commercial tanning lamps and beds can cause age spots.
We offer a range of advanced laser therapies tailored to the type and depth of discoloration, whether you’re dealing with brown spots, melasma, sun damage, or red marks from acne or rosacea. Each treatment is selected based on your unique skin tone, condition, and goals.
Lasers for Brown Spots, Melasma & Sun Damage:
These lasers use ultra-short pulses to break up unwanted pigment while minimizing damage to surrounding skin, ideal for darker skin tones.
Q-switched Nd:YAG Laser: Targets deep pigmentation, including melasma and post-inflammatory hyperpigmentation (PIH), with precision and safety for all skin tones.
Fractional Lasers: These versatile lasers treat pigmentation and improve overall skin quality by stimulating collagen production and resurfacing the skin. Great for: PIH (post inflammatory hyperpigmentation), sun damage, acne scarring, uneven tone, and texture.
Vascular Lasers:
Specialized for redness and pink-toned PIH (post inflammatory hyperpigmentation), especially from acne or rosacea.
Vbeam (Pulsed Dye Laser):
Targets blood vessels to reduce red marks, flushing, and inflammation. A gentle, effective option for sensitive or reactive skin types.
Each laser treatment is customized to your skin’s needs to ensure safe, effective results. During your consultation, we’ll determine the best approach—often combining laser therapy with topical treatments to maximize improvement and minimize recurrence.
For brown marks on deeper skin tones, we use a combination of hydroquinone, kojic acid, Vitamin C, and AHAs to gently and effectively lighten dark spots while brightening and smoothing the skin.
These clinically proven ingredients work synergistically to visibly brighten, lighten, and tighten the skin, revealing a more even, radiant complexion.
JAS Anti - Aging TRIO, expertly formulated to replenish, exfoliate, and restore your skin’s natural glow.
To help avoid age spots and new spots after treatment, follow these tips for limiting your sun exposure:
⚠️ Important
Always see a board-certified dermatologist or laser specialist, especially if you have darker skin.
Sun protection is non-negotiable—exposure after treatment can trigger new pigment.
If you are tired of looking older or want the spots removed, schedule a laser consultation and restore your skin to its natural beauty. Our Cosmetic Consultation Reimbursement policy is offered to all patients. Schedule an office visit to discuss your concerns and skincare goals with Dr. Robinson and the office visit cost will be applied to the future cost for the "consulted procedure". The "consulted procedure" must be completed within 30 days of your consult visit.
Birthmarks are abnormalities of the skin that are present when a baby is born.
A birthmark can be red or brown.
A red or vascular birthmark is made up of dilated blood vessels. Two types are hemangiomas and port-wine stains. Although they can resolve spontaneously on their own, some can cause deformities and become more purple in color. With the advent of laser treatment, the Nevus Flameus can be cleared and subsequent deformities prevented.
A Nevus of Ota, Nevus of Ito and Mongolian spot are brown to bluish birthmarks that usually occur around the eye, shoulder and trunk respectively. Given their size and location patients often consider them cosmetically unacceptable, using the Medlite Nd:Yag laser these birthmarks can be treated effectively with excellent results.
An atypical nevus or dysplastic nevus (mole) is a benign growth that may share some of the features of a melanoma, but is NOT a melanoma or any other form of cancer. The presence of an atypical nevus, however, may increase the risk of developing a melanoma, or be a marker for it. A single atypical nevus may indicate a small risk; this risk increases with the number of atypical nevi present.
An atypical nevus can vary in appearance. Since it has the ABCDE features of a melanoma, it is important ot have a dermatologist examine all moles.
Asymmetry - One half does not match the other half in size, shape, color, or thickness.
Border irregularity - The edges are ragged, scalloped, or poorly defined.
Color - The pigmentation is not uniform. Shades of tan, brown, and black are present. Dashes of red, white, and blue add to the mottled appearance.
Diameter - While melanomas are usually greater than 6mm in diameter (the size of a pencil eraser) when diagnosed, they can be smaller. If you notice a mole different from others, or one which changes, itches, or bleeds (even if it is small), you sould see a dermatologist.
The lifetime risk of a person in the United States developing melanoma is 1 in 75. A patient with one to four atypical nevi without a personal or family history of melanoma is at a slightly higher risk than the general population. The risk of developing melanoma is higher if a patient with atypical nevi has a personal or family history of melanoma. A patient who has multiple atypical and normal nevi (moles) may have Familial Atypical Nevus Syndrome, and is at an increased risk for developing a melanoma, especially if a relative had melanoma.
Where and when do atypical nevi occur?
Atypical nevi begin to appear at puberty and can occur anywhere on the body, but are more common in sun-exposed areas, the back, and the legs.
Since an atypical nevus is not the same as a melanoma, it does not need to be treated aggressively but should be observed for changes, biopsied, or conservatively excised.
Familial Atypical Nevus Syndrome
The National Institute of Health Consensus Conference defines the Familial Atypical Nevus Syndrome as those persons meeting the following criteria:
It is important for people with Familial Atypical Nevus Syndrome to have a full body screening from a dermatologist every three to twelve months beginning with the onset of puberty. The dermatologist might also recommend regular ophthalmologic examinations, baseline skin photography, or regular screenings of relatives to permit early detection and treatment of melanoma since detection in the early stages has a much higher cure rate.
People with Familial Atypical Nevus Syndrome should also examine their own skin every month. When performing self-examinations, be aware of any lesions that appear to change in size, color, and/or shape. If a change has occurred, bring this to the attention of a dermatologist immediately. Information on the early signs of melanoma is available from the dermatologist or the American Academy of Dermatology.
Prevention of Melanoma
Alopecia areata (AA) causes hair loss in small, round patches that may go away on their own, or may last for many years. Nearly 2% of the U.S. population (about four million people) will develop AA in their lifetime. Some people with AA (about 5%) may lose all scalp hair (alopecia totalis) or all scalp and body hair (alopecia universalis). It is an autoimmune disease, in which for unknown reasons your immune system attacks your own hair follicles, (where the hair grows from), resulting in damage that leads to hair loss anywhere on the body. Typically, it affects small patches of hair so, it may go completely unnoticed. However, more patches of hair loss could develop close together, making it more noticeable.
AA occurs world-wide in both genders and in every ethnic group. Children and young adults are most frequently affected, but persons of all ages are susceptible. One in five persons with AA has a family member who also has the disease.
AA usually begins with one or more small, round, coin-size, bare patches. It is most common on the scalp, but can involve any hair-bearing site on the body including eyebrows, eyelashes, and beards. Hair may fall out and regrow with the possibility of full hair regrowth always present. AA usually has no associated symptoms, but there may be minor discomfort or itching prior to developing a new patch. Nails may have tiny pinpoint dents, ridges, become brittle and may, in rare instances, become distorted.

AA is not contagious. It is an autoimmune disease in which the body's immune system attacks itself, in this case, the hair follicles. The cause is not known. A person's particular genetic makeup combined with other factors triggers AA.
The main types are:
Alopecia areata: Alopecia is the medical term for bald. Areata means patchy. This patchy baldness can develop anywhere on the body, including the scalp, beard area, eyebrows, eyelashes, armpits, inside your nose, or ears.
Alopecia totalis: The person loses all hair on the scalp, so the scalp is completely bald.
Alopecia universalis: The person loses all hair, leaving the entire body hairless. This is rare.
Although your dermatologist may know by examining your scalp that you have AA, occasionally, a scalp biopsy is helpful in confirming the diagnosis.
Because there are so many reasons for hair loss, testing is sometimes necessary to make sure alopecia areata is the cause of your hair loss.
A blood test can look for other diseases caused by the immune system. Sometimes, other tests are necessary.
AA is not a symptom of a serious disease and usually occurs in otherwise healthy individuals. Persons with AA may have a higher risk of atopic eczema, asthma, and nasal allergies, as well as other autoimmune diseases such as thyroid disease (Hashimoto's thyroiditis), and vitiligo. Family members may also have atopic eczema, asthma, nasal allergies, or autoimmune diseases (i.e. insulin-dependent diabetes, rheumatoid arthritis, thyroid disease, or systemic lupus erythematosus).

Yes, it is likely that the hair may regrow, but it may fall out again. The course of the disease varies from person to person, and no one can predict when the hair might regrow or fall out again. This unpredictability of AA, and the lack of control over it, makes this condition frustrating. Some people lose a few patches of hair, the hair regrows, and the condition never returns. Other people continue to lose and regrow hair for many years. The potential for full regrowth is always there, even in people who lose all the hair on their scalp and body (alopecia totalis/universalis). Hair could regrow white or fine, but the original hair color and texture may return later.
The good news is that many causes of hair loss can be managed when caught early and further loss can usually be slowed or prevented.
Corticosteroids are anti-inflammatory drugs that suppress the immune system. They can be given as injections into the areas of hair loss, rubbed topically into affected areas or taken orally as pills.
Oral Minoxidil is by prescription only. Dermatologists began using low-dose oral minoxidil for hair loss after noticing the side effects of the high-dose version of the drug used to treat high blood pressure increased hair growth. The efficacy of 5mg oral minoxidil for men with androgenetic alopecia was tested. Researchers concluded that 43% of the patients had excellent results in hair growth. Typically, people prefer oral to topical. They find it easier and more convenient to take the medication orally, may be able to save money with an oral minoxidil prescription and prefer not to have residue on their hair.
Topical Minoxidil 5% Solution aka Rogaine solution or foam is available over the counter. Effectiveness of topical Minoxidil works for about 2 out of 3 men. It's most effective if you're under age 40 and have only recently started to lose your hair. How to use it: Twice a day, when your hair is dry, apply minoxidil on your scalp where the hair has started to thin. Minoxidil can help maintain the regrowth after you stop applying the corticosteroid. It has few side effects, so it’s considered a good option for children. New hair growth may appear in about 12 weeks.
PRP (platelet-rich plasma) therapy for hair loss is a three-step medical treatment in which a person’s blood is drawn, processed, and then injected into the scalp.
PRP injections trigger natural hair growth and maintain it by increasing blood supply to the hair follicle and increasing the thickness of the hair shaft. Sometimes this approach is combined with other hair loss procedures or medications.
PRP therapy is a three-step process. Most PRP therapy requires three treatments 4–6 weeks apart.
Maintenance treatments are required every 4–6 months.
Your blood is drawn — typically from your arm — and put into a centrifuge (a machine that spins rapidly to separate fluids of different densities).
After about 10 minutes in the centrifuge, your blood will have separated into in three layers:
The platelet-rich plasma is drawn up into a syringe and then injected into areas of the scalp that need increased hair growth.
There hasn’t been enough research to prove whether PRP is effective. It’s also unclear for whom — and under what circumstances — it’s most effective.
Wigs, caps, hats, or scarves are important options. Wearing a head covering does not interfere with hair regrowth. This may be a good choice for people with extensive scalp hair loss who do not have enough hair to cover it.
The emotional aspects of living with hair loss can be challenging, especially in a society that regards hair as a sign of youth and good health. It is reassuring that alopecia areata does not affect general health, and should not interfere with your ability to achieve all of your life goals at school, in sports, in your career, and in raising a family.
The National Alopecia Areata Foundation, the NAAF, is a great resource for support, treatment & education.
Schedule an appointment to see which treatment or combination of treatments is the best choice for you.
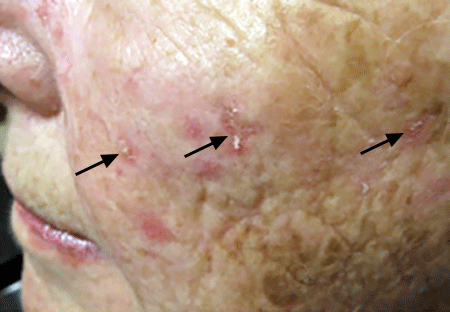
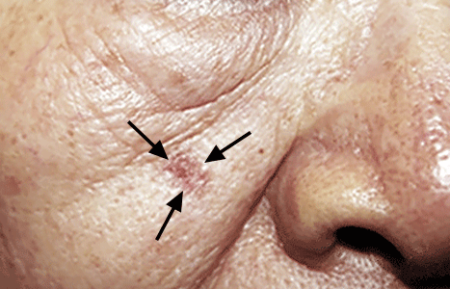
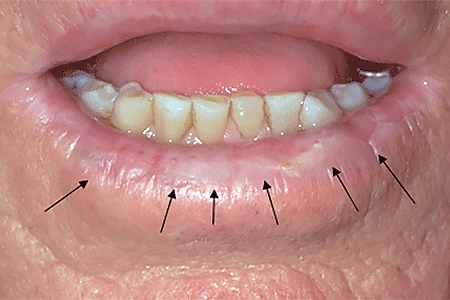
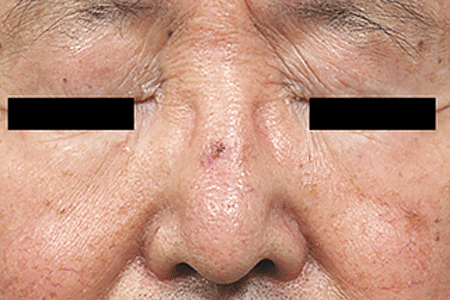
An actinic keratosis, is a rough, scaly patch on the skin that develops from years of sun exposure. It's often found on the face, lips, ears, forearms, scalp, neck or back of the hands. These represent pre-cancerous growths that can become skin cancer if left untreated.
If you find a spot or growth on your skin that you think could be an actinic keratosis (AK), it’s time for a thorough skin exam. Should you have an AK, an accurate diagnosis and treatment can:
Most people who have AKs (or think they may have an AK) see a dermatologist. This is actually one of the most common conditions that dermatologists diagnose and treat.
When you see a board-certified dermatologist about AKs, your dermatologist will:
If you have one or more AKs on your skin, a board-certified dermatologist can often diagnose you by looking carefully at your skin. While examining your skin, your dermatologist will also look for signs of skin cancer. People who have skin that’s been badly damaged by ultraviolet (UV) light develop AKs and have a higher risk of getting skin cancer.
If you have one or more AKs, your dermatologist will talk with you about whether to treat these precancerous skin growths. Usually, treatment is recommended.
For a few people, a dermatologist may recommend frequent skin exams rather than treatment. Skin exams are recommended for patients who are frail and may find it hard to tolerate treatment. To be effective, treatment must destroy the AKs. When this happens, your skin will feel raw. It may be red and swollen for a brief time.
The treatment that is right for you depends on several considerations, including:
If you have one or a few AKs, a procedure that your dermatologist can perform during an appointment may be the preferred treatment.
You can often complete treatment in 1 or 2 office visits. The procedures that dermatologists use to treat AKs include:
Some people develop a few AKs, which can often be cleared with treatment.
If you have many AKs, it’s a good idea to be under a dermatologist’s care. Your skin has been severely damaged by UV light, so it’s likely you’ll continue get new AKs. You may also develop skin cancer. Your dermatologist can watch for signs of new AKs and skin cancer. When found early and treated, skin cancer is highly treatable.
Your dermatologist will tell you how often to return for check-ups. Some people need a check-up once or twice a year. If you have a weakened immune system or a rare condition that greatly increases your risk of developing AKs and skin cancer, you may need to see your dermatologist every 8 to 12 weeks.
Keep every appointment. If skin cancer develops, the sooner it is found and treated, the better your outcome.
Self-care also plays a key role in your outcome. The right self-care can help to prevent new AKs and skin cancer.


Acne is a skin condition which has plugged pores (blackheads and whiteheads), inflamed pimples (pustules), and deeper lumps (nodules). Acne occurs on the face, as well as the neck, chest, back, shoulders, and upper arms. Although most teenagers get some form of acne, adults in their 20's, 30's, 40's, or even older, can develop acne. Often, acne clears up after several years, even without treatment. Acne can be disfiguring and upsetting to the patient. Untreated acne can leave permanent scars; these may be treated by your dermatologist in the future. To avoid acne scarring, treating acne is important.
Acne is not caused by dirt. Testosterone, a hormone which is present in both males and females, increases during adolescence (puberty). It stimulates the sebaceous glands of the skin to enlarge, produce oil, and plug the pores. Whiteheads (closed comedones), blackheads (open comedones), and pimples (pustules) are present in teenage acne.
Early acne occurs before the first period and is called prepubertal acne. When acne is severe and forms deep "pus-filled" lumps, it is called cystic acne. This may be more common in males. Adult acne develops later in life and may be related to hormones, childbirth, menopause, or stopping the pill. Adult women may be treated at the period and at ovulation when acne is especially severe, or throughout the entire cycle. Adult acne is not rosacea, a disease in which blackheads and whiteheads do not occur.
Acne has nothing to do with not washing your face. However, it is best to wash your face with a mild cleanser and warm water daily. Washing too often or too vigorously may actually make your acne worse.
Acne is not caused by foods. However, if certain foods seem to make your acne worse, try to avoid them.
Wear as little cosmetics as possible. Oil-free, water-based moisturizers and make-up should be used. Choose products that are "non-comedogenic" (should not cause whiteheads or blackheads) or "non-acnegenic" (should not cause acne). Remove your cosmetics every night with mild soap or gentle cleanser and water.
A flesh-tinted acne lotion containing acne medications can safely hide blemishes. Loose powder in combination with an oil-free foundation is also good for cover-up.
Shield your face when applying sprays and gels on your hair.
Control of acne is an ongoing process. All acne treatments work by preventing new acne breakouts. Existing blemishes must heal on their own, and therefore, improvement takes time. If your acne has not improved within two to three months, your treatment may need to be changed. The treatment your dermatologist recommends will vary according to the type of acne.
Occasionally, an acne-like rash can be due to another cause such as make-up or lotions, or from oral medication. It is important to help your dermatologist by providing an updated history of what you are using on your skin or taking internally.
Many non-prescription acne lotions and creams help mild cases of acne. However, many will also make your skin dry. Follow instructions carefully.
Re-think your skin health. Hydrafacial MD, - * Acne Facial, is highly effective for anyone suffering from oily and/or acne-prone skin. It visibly reduces redness, enlarged pores, hyperpigmentation, utilizing LED blue light killing acne causing bacteria. HydraFacial MD - Hydradermabrasion is the latest, non-invasive, "gentle" skin resurfacing and complexion treatment. The immediate, noticeable, long lasting results are achieved with zero downtime and without any discomfort. You can return to school, work, social life, or exercise right after your procedure. HydraFacial MD uses a uniquely shaped spiral tip and patented vortex fusing technology to gently cleanse, exfoliate, and extract, removing impurities and dead skin cells while hydrating the skin and adding antioxidant protection simultaneously.
Acne scars no longer have to be lived with forever. Often occurring on the face, back and chest these scars can now be treated with a variety of lasers (Fraxel®, V-Beam), subcission or chemical peels. These treatments require no social downtime and can be performed on all skin colors.
XEOMIN is a botulinum toxin that has been used internationally since 2005 and was introduced to the US market in 2010 by Merz Pharmaceuticals, LLC. The FDA recently approved Xeomin for the treatment of severe frown lines.
Xeomin is similar to other treatments such as Botox, but has it's own advantages, beginning with the fact that it contains no additives, just botulinum toxin type A. This may mean that there is less risk of developing antibodies against Xeomin than other available neurotoxins. The body develops antibodies in response to a foreign invader and attacks. In theory, antibodies could prevent a neurotoxin from having its desired effects.
The full effects of Xeomin occur within one week, and the results last from three to six months, making it comparable to Botox in terms of both onset and duration of action. Xeomin prices are also quite competitive to existing botulinum toxin therapies.
Dr Robinson offers Xeomin treatments, and would be happy to discuss with you whether Xeomin is the right approach to help you to look more youthful. Dr. Robinson's training and expertise will enable you to make the best possible decisions regarding your health and appearance during a cosmetic consultation.

